


Introduction: Patients with relapsed and refractory multiple myeloma (RRMM) who are triple-class exposed to immunomodulatory drugs, proteasome inhibitors, and anti-CD38 antibodies have poor clinical outcomes. Idecabtagene vicleucel (ide-cel, bb2121) is a chimeric antigen receptor (CAR) T cell therapy under development for this patient population. The ide-cel construct includes a single-chain variable fragment anti-B-cell maturation antigen (BCMA) recognition domain, a CD3-zeta activation domain, and a 4-1BB T-cell activation domain. An ongoing, single-arm phase 2 study to evaluate the efficacy and safety of ide-cel in RRMM (KarMMa; NCT03361748) reported an overall response rate (ORR) of 73%, a complete response rate of 31%, a median duration of response of 10.6 months, median progression-free survival (PFS) of 8.8 months, and a median overall survival (OS) of 19.4 months in the treated population (Munshi NC, et al. J Clin Oncol 2020;38:8503). A systematic literature review of published efficacy data for triple-class-exposed patients with RRMM identified MAMMOTH, a large, retrospective observational study (Gandhi UH, et al. Leukemia 2019;33:2266-2275). Patients in both MAMMOTH and KarMMa were triple-class exposed. In MAMMOTH, patients received a variety of regimens corresponding to conventional care (CC) following progression on anti-CD38 antibodies. This analysis aimed to compare efficacy outcomes observed with ide-cel treatment in KarMMa and CC in MAMMOTH.
Methods: Individual patient-level data (IPD) with a median follow-up of 13.3 months were available for KarMMa (data cutoff January 14, 2020) while study-level data were available for MAMMOTH. Unanchored matching-adjusted indirect comparisons (MAICs) were conducted to compare efficacy outcomes from the 2 studies. These analyses were performed on data from 128 patients who received ide-cel (target dose 150, 300, or 450 × 106 CAR+ T cells) in KarMMa, and 249 patients who received CC therapies after progression on an anti-CD38 antibody in MAMMOTH. IPD from MAMMOTH were reconstructed based on published Kaplan-Meier curves for time-to-event outcomes. The most relevant differences in patient characteristics between the studies were identified for adjustment based on published literature and clinical expertise. These included the number of prior lines of treatment, proportion of patients refractory to specific prior treatments, and time since diagnosis. Propensity score models were used to weight the treated population from KarMMa to match the baseline characteristics of treated patients in MAMMOTH in order to predict outcomes for ide-cel in a population corresponding to those evaluated in MAMMOTH. The effective sample size (ESS) was calculated as a measure of the amount of overlap between the study populations included in the MAIC. Odds ratios (ORs) were calculated for ORR using weighted logistic regression models. Hazard ratios (HRs) were calculated for PFS and OS using weighted Cox proportional hazards models.
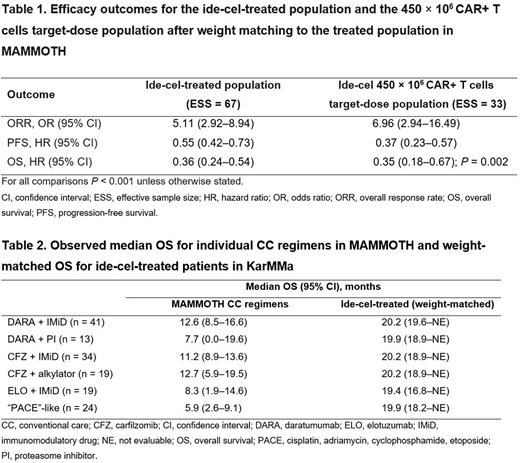
Results: Ide-cel was associated with a significantly higher ORR compared with CC in a population matched to the treated MAMMOTH population (OR 5.11, 95% confidence interval [CI] 2.92-8.94, P < 0.001) (Table 1). Similarly, ide-cel significantly extended PFS (HR 0.55, 95% CI 0.42-0.73, P < 0.001) and OS (HR 0.36, 95% CI 0.24-0.54, P < 0.001) versus CC. Results were generally consistent for patients in the ITT population and those who received the target dose of 450 × 106 CAR+ T cells who experienced efficacy gains exceeding those receiving lower target doses. In MAMMOTH, the individual CC regimens involving targeted therapies (carfilzomib, daratumumab, and elotuzumab) were associated with a median OS of between 8.3 and 12.7 months. The weighted median OS times for ide-cel are consistently longer than those associated with the individual CC regimens in MAMMOTH (Table 2), similar to the results for the overall treated population. Limitations of this inter-study comparison include a tighter window of OS evaluation in the ide-cel arm, which may have underestimated the true difference. More broadly, there is also a risk of bias given limited reporting on potential confounders.
Conclusion: Ide-cel provides clinically and statistically significant efficacy benefits over current CC, including combination regimens involving targeted agents.
Shah:GSK, Amgen, Indapta Therapeutics, Sanofi, BMS, CareDx, Kite, Karyopharm: Consultancy; BMS, Janssen, Bluebird Bio, Sutro Biopharma, Teneobio, Poseida, Nektar: Research Funding. Ayers:PRECISIONheor: Current Employment. Davies:Adaptive Biotech: Honoraria; Sanofi: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene/BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncopeptides: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Cope:PRECISIONheor: Current Employment. Mojebi:PRECISIONheor: Current Employment. Parikh:BMS: Current Employment, Current equity holder in publicly-traded company. Dhanda:BMS: Current Employment, Current equity holder in publicly-traded company. Hari:Amgen: Consultancy; Janssen: Consultancy; GSK: Consultancy; Takeda: Consultancy; Incyte Corporation: Consultancy; BMS: Consultancy. Patel:BMS: Current Employment. Huang:BMS: Current Employment, Current equity holder in publicly-traded company. Hege:BMS: Current Employment, Current equity holder in publicly-traded company, Other: Travel, accommodations, expenses, Patents & Royalties: Numerous, Research Funding; Mersana Therapeutics: Current equity holder in publicly-traded company, Membership on an entity's Board of Directors or advisory committees; Arcus Biosciences: Divested equity in a private or publicly-traded company in the past 24 months. Dhanasiri:BMS: Current Employment, Current equity holder in publicly-traded company.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal